
Hi everyone, it has been a while. We are finally back in action; assessing, treating and OTing ! I am now placed at a chronic facility which is completely different to the previous acute facility. The pace, atmosphere and time frame of conditions have changed therefore I have realized I also need to change the way I think and approach treatment. The topic for today is the clinical reasoning cycle, it has assisted me with this change of mindset.
So what exactly is the clinical reasoning cycle ?
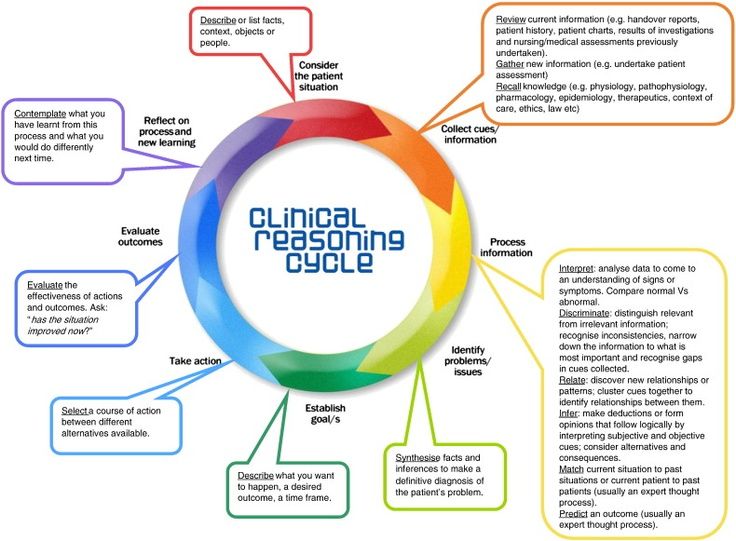
It is the process by which health care workers collect cues, process the information, come to an understanding of a patient problem or situation, plan and implement interventions, evaluate outcomes, and reflect on and learn from the process (Hoffman, 2007; Kraischsk & Anthony, 2001; Laurie et al.,2001).
And what is it importance of clinical reasoning ?
According to () it is an important skill to develop and if it is implemented correctly it will have a positive impact on the patient’s outcomes. The clinical reasoning cycle is a process which helps health care workers provide the best possible therapy to patients.
How have I put clinical reasoning into practice you ask ?
I have considered my patient in their situation, as I know she is a 33 year old female who is a paraplegic and she had sustained a T11/12 fracture by falling. I was able to gather the information through conducting an interview and reading the patients file. The next step involved collecting information on the clients abilities in occupations, performance skills and performance context through preforming standardized assessments, functional based assessments and observations. (For example, I observed the patient is not able to sit on the edge of the bed without using her hands as support.) Once collecting the information from the assessments, it is processed and interpreted by comparing the assessment findings of the patient against the norms. (She therefore has impaired static sitting balance). Integrated problem statements are then created and used to establish goals. (The impaired balance affects her ability to participate in occupations independently such as transferring therefore an aim can be to improve balance.) Taking action involves preforming a treatment session with the patient. (I did a table top activity with the client on a bench, no back support to strengthen trunk muscles to improve balance.) Evaluation of the effectiveness of treatment and reflection will be done after the block.
The second topic for today is cultural humility. “In the medical context, cultural humility may be defined as a process of being aware of how people’s culture can impact their health behaviors and in turn using this awareness to cultivate sensitive approaches in treating patients” (Prasad et al., 2016). I practiced cultural humility during sessions because it helps when developing a rapport with patients. It also will help to understand the patient’s behavior when observing them performing tasks.
Reflection on treatment session:
After completing the relevant assessments I decided to the aim of intervention would be improving the clients impaired performance components such as balance, physical endurance, muscle strength of the upper limb and equilibrium reactions and postural control which would in turn increase the clients independence in occupations. One treatment session consisted of a wheelchair obstacle course which involved the patient moving through cones and up a ramp to improve physical endurance and muscle strength of the upper limbs. The patient was able to complete the session without difficulty, therefore upgrading should have been implemented. The structuring of the activity could have been adapted to increase the amount of resistance to improve the performance skills targeted. For example self propelling over grass. The number of repetitions for performing the course could have been increased to build endurance.
Reflection on feedback:
I learnt the importance of knowing when to use occupation as a mean vs occupation as an end. As well as how these two concepts will impact how one writes the principles of the session. I will apply the information gather from the feedback into the next week of prac ! Also an important point is to validate your assessment finding statement with a standardized measure to ensure the correct interpretation of your assessment finding notes by other health care workers.
References:
1. Hughes, R., Benner, P., & Sutphen, M. (2008). Patient safety and quality (Chapter 6Clinical Reasoning, Decisionmaking, and Action: Thinking Critically and Clinically). Rockville, MD: Agency for Healthcare Research and Quality.
2. (2020). Retrieved 15 July 2020, from https://www.utas.edu.au/__data/assets/pdf_file/0003/263487/Clinical-Reasoning-Instructor-Resources.pdf
3. Waters, A., & Asbill, L. (2013). Reflections on cultural humility. Retrieved 15 July 2020, from https://www.apa.org/pi/families/resources/newsletter/2013/08/cultural-humility
4. Prasad, S., Nair, P., Gadhvi, K., Barai, I., Danish, H., & Philip, A. (2016). Cultural humility: treating the patient, not the illness. Medical Education Online, 21(1), 30908. doi: 10.3402/meo.v21.30908
University of Natal, Pietermaritzburg
Links: https://hogg.utexas.edu/3-things-to-know-cultural-humilit
